This is the first article of the two on adolescent pregnancy that addresses causes of adolescent pregnancy. In our second article we cover the effects of adolescent pregnancy and recommendations for the government of Turkmenistan to tackle adolescent pregnancy.
At this year’s CEDAW session, the Turkmenistan delegation indicated a positive downward trend in adolescent pregnancies, citing that in 2022 it was 22.9 births per 1000 girls, while in 2019 it was 24.5. It is not clear which sources the government is attributing to. However, based on the 2019 MICS there were already 22 pregnancies per 1000 girls aged 15-19, in the meantime UNFPA in Turkmenistan indicates 27 pregnancies per 1,000 girls aged 15-19 every year as of 2023. Indeed since 2016 MICS submission, the trend went down from 28 pregnancies per 1000 girls aged 15-19. Nevertheless, due to inconsistencies with the data, it is hard to assess it as a positive downward trend. It is rather fluctuating with no significant meaningful changes.
Despite these irregularities, adolescent pregnancy is relatively low in Turkmenistan compared to the neighboring Central Asian countries. Factors contributing to adolescent pregnancy include limited access to sexual and reproductive health information and services, early and forced marriages, and socio-economic pressures. The biggest issue in Turkmenistan remains a significant gap in unmet need for family planning among girls and comprehensive education on contraception and gender-based violence.
Women who are married before age 18 tend to have more children than those who marry later in life. Pregnancy-related deaths are known to be a leading cause of mortality for both married and unmarried girls aged 15-19, particularly among the youngest of this cohort. Evidence suggests that girls who marry at young ages are more likely to marry older men, which puts them at increased risk of HIV infection. The demand for this young wife to reproduce, and the power imbalance resulting from the age differential, lead to very low condom use among such couples.
Overall, adolescent pregnancy is on the decline in Eastern Europe and Central Asia, but the issue still persists and impacts the girls differently depending on the country, social-economic status, education and regions within countries. In this article, we will look into the situation of adolescent pregnancy in Turkmenistan in more detail and try to understand what can be done to curb this trend and protect human rights and well-being of girls in Turkmenistan, as well as ensure non-discriminatory access to maternal health care for adolescents.
The information and insights in this article have been drawn from a variety of sources, including international organizations, open sources, and available data. It is important to note that the Turkmenistan government has limited official information and statistics on adolescent pregnancy, and does not have research on the root causes and potential solutions to this issue. Therefore, much of the analysis presented here is based on the expertise and research conducted by international organizations, NGOs, and global health institutions. These sources include the Guttmacher Data, UNICEF MICS 2019, WHO, UNFPA, 2023 Voluntary National Review of Turkmenistan, and the 2022 Common Country Analysis report, among others.
What is adolescent pregnancy?
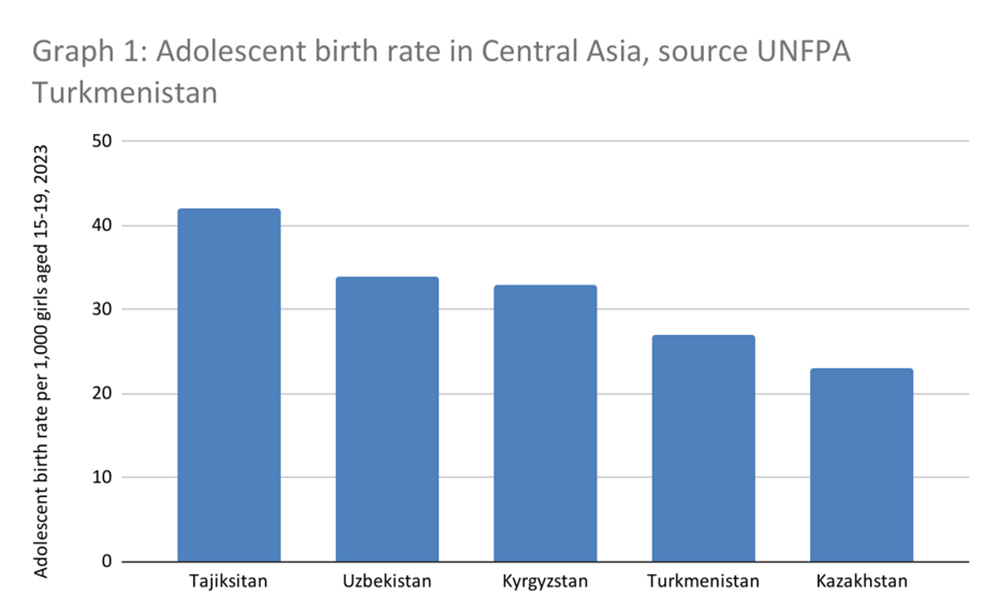
Also known as teenage or teen pregnancy, adolescent pregnancy is a global phenomenon that affects young girls between the ages 15-19, but it can include girls as young as 10. Turkmenistan positions second lowest after Kazakhstan in Central Asia, in adolescent pregnancy, as for 1,000 girls aged 15-19, there were 27 pregnancies in 2023 (Graph 1).
This may seem low, but in total, there are around 5500 adolescent girls between the ages 15-19, who give birth each year in Turkmenistan.
Addressing adolescent pregnancy is part of the Sustainable Development Goals including under indicators 3.7.1 “Proportion of women of reproductive age (aged 15-49 years) who have their need for family planning satisfied with modern methods”, 3.7.2, “Adolescent birth rate (aged 10–14 years; aged 15–19 years) per 1000 women in that age group,” and 5.3.1, “Proportion of women aged 20–24 years married before the age of 18 years”.
The causes of adolescent pregnancy
There are different reasons why young girls become pregnant. Among them are lack of information about sexual and reproductive health and rights, inadequate access to services tailored to young people, family, community and social pressure to marry and start a family, sexual violence, and early child and forced marriage, which can be both a cause and a consequence of adolescent pregnancy. However, as of today, there is no specific study in Turkmenistan that looks into causes and effects of adolescent pregnancy.
Socio-economic factors
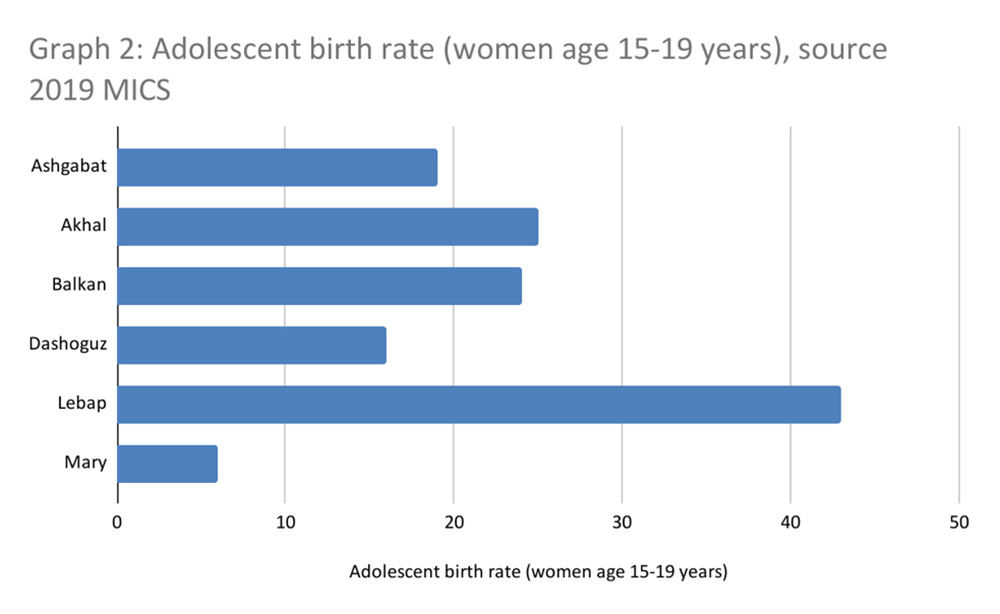
Adolescent pregnancy disproportionately impacts those with less education or of low economic status. For example, in Turkmenistan in urban areas this indicator was 20.4, while in rural areas – 25.0. Similarly, Lebap velayat has the most unfavorable picture in terms of adolescent pregnancy indicators and is among the poorest regions in the country based on the MICS 2019 survey (Graphs 2 and 3). Lebap also scored the highest in child marriage, followed by Akhal velayat in both indicators, supposedly the most conservative region in the country.

Approximately 90% of births among girls aged 15-19 in developing countries occur within early marriage where there is often an imbalance of power, no access to contraception and pressure on girls to prove their fertility. In Turkmenistan, child marriage by age 18 in 2006-2022 constituted 6%. There is an apparent parallel in the country between the two, as adolescent pregnancy happens more often in those areas where more girls get married early, and most likely similar socio-economic factors lead to both issues (Graph 4).

Bodily autonomy and decision making
Married young girls have the lowest agency and less control to make independent decisions about their bodies and pregnancy. In Turkmenistan, over 52% of the girls aged 15-19 cannot refuse to have sexual intercourse with their husband/partner, and only 10% of women aged 15-19 make their own informed decisions regarding sexual relations, contraceptive use and reproductive health care. Moreover, 1 out of 3 married girls have partners who are 5 or more years older than them.
Donate to support Turkmen analysts, researchers and writers to produce factual, constructive and progressive content in their efforts to educate the public of Turkmenistan.
SUPPORT OUR WORKIn the meantime, state media promotes pronatalist propaganda encouraging women in Turkmenistan to have eight children. Macho politics, health misinformation and abortion stigma are the norms. Family values in the name of maintaining tradition promotion also enables the control of women’s bodies and population growth. Ongoing reports by independent media mention periodic government campaigns to subject adolescent girls at schools to gynecological exams and most likely virginity tests. Although, it is not clear if this is done as prevention and with girls consent or these are forced tests, it is important to underline that according to the UN and WHO, virginity testing are considered human rights violations.
Indirectly all mentioned factors set the tone of the women’s roles and place in the society for young girls. Besides, from a younger age women have less opportunities as parents invest financially more in their sons in Turkmenistan. Among these investments is education. It is also not clear what happens to girls when they get pregnant and while being at school: do they drop out of school or they complete their education and what is the probability of either of the scenarios for the girls? It is certain, however, that in expected and mean years of schooling Turkmenistan has one of the largest differences between women and men in Central Asia, with average years of schooling for boys being 11.6 years and for girls it is 10.9 years. Promotion of motherhood and marriage and limited options for girls to realize themselves have a significant socio-emotional and economic impact on girls, leaving limited paths for growth.
Contraception and abortion policies
Child marriage places girls at increased risk of pregnancy, often unintended. In many places, barriers to obtaining and using contraceptives prevent adolescents from avoiding unintended pregnancies. For example, out of 5,500 adolescent girls who give birth each year in Turkmenistan, 3,600 want to avoid pregnancies. While Turkmenistan may have the lowest percent of annual adolescent pregnancy per all birth cases in the region, and girls know at least about one contraception, Turkmenistan has the highest percentage of girls in the region whose needs for contraception and family planning are not met (88%) (Graph 5).

Currently in Turkmenistan, there are only seven modern contraceptive methods, such as combined oral contraceptives, progestogen only pills, Copper‐bearing IUDs, DMPA injectables, NET‐EN injectables, male condoms and female condoms. These contraceptive methods are offered by primary health care units, reproductive health consultation rooms, hospitals and HIV centers. In total, there are 95 public reproductive health consultation rooms providing family planning services across Turkmenistan. However, there are no private non‐profit or non‐governmental organizations providing family planning services.This means the 95 public health institutions are supposed to meet the needs of over 1,5 million women of reproductive age in Turkmenistan, including around 8% of population aged 15-19, which is approximately 260,000 girls. And as stated by the UNFPA investment case study on family planning, while these institutions offer family planning services, access and quality of services is uneven, often leaving women with disabilities and young people in rural areas behind.
In 2018 the Ministry of Health of Turkmenistan adopted a strategy to monitor adolescent reproductive health. Same year, adolescent girls were also included in the list of eligible groups for contraceptives uptake free of charge, as well as into the list of most at-risk women eligible for reproductive health commodities in the above-mentioned 95 reproductive health rooms countrywide. While contraceptives are free‐of‐charge for all the target vulnerable groups, including the last fourth group of women between 15‐19 years of age, sexually active and needing contraception, in practice contraceptive services are free‐of‐charge only for a narrow group of women who have medical conditions which put them at risk of death or deteriorating their health condition due to the unplanned pregnancy (second‐ and third‐ degree of liver, heart, kidney, liver failure, cirrhosis, heart attack, second and third degree of hypertension, and glomerulonephritis). For the rest of women in the target group, contraceptive services are charged, but with a low price. In addition, access to free services may incur travel costs and opportunity costs (not working at the time women receive the services), which means that for many young girls these services are mostly inaccessible.
In general, the lack of family planning is higher for women in rural areas (54%), in the poorest quintile (53%) and for women with only primary or secondary education level (51%) in Turkmenistan.
In 2013 the Law on State Youth Policy now promotes and guarantees youth participation, access of adolescents and youth to youth-friendly reproductive health services, HIV and AIDS prevention and volunteerism. And according to the 2022 Common Country Analysis report, the government of Turkmenistan works on creating and strengthening youth-friendly healthcare services as a priority within the framework of the National Strategy on Reproductive, Maternal, Newborn, Children and Adolescent Health for 2021-2030. Despite these efforts, the unmet need for family planning is still high among the girls aged 15-19 in Turkmenistan.
Studies also show that even when adolescents can obtain contraceptives, they may lack the agency or the resources to pay for them, knowledge on where to obtain them and how to correctly use them. Adolescents may also face stigma when trying to obtain contraceptives. Also, they are often at higher risk of discontinuing use due to side effects, and due to changing life circumstances and reproductive intentions. This is often combined with health worker bias and/ or lack of willingness to acknowledge adolescents’ sexual health needs, which in traditional environments, like Turkmenistan, young girls, unless married, may face quite often. And in countries with restrictive abortion laws, young girls may be either be pressured or forced to give birth. Such trends only contribute to a number of unintended pregnancies and adolescent pregnancies overall in the country.
When it comes to abortion policy, Turkmenistan’s has the lowest gestational limit on abortion in the world limiting abortion up to 5 weeks only. The current Public Health Care Act is a regression on the previous law which allowed pregnancy up to 12 weeks of gestation. Under the country’s Criminal Code, abortion is allowed only in state medical institutions. And if performed beyond the legal grounds, a qualified provider may be imprisoned for up to 2 years. The current law also requires parental written consent and a medical advisory commission decision for abortions involving pregnant minors including those up to 5 weeks of pregnancy. Lastly, while self-managed abortion is not expressly prohibited under the Criminal Code, it may still be interpreted as an offense and subject the women to imprisonment.
For many adolescents, pregnancy and childbirth are neither planned, nor wanted. In countries where abortion is prohibited or highly restricted, adolescents typically resort to unsafe abortion, putting their health and lives at risk. With changes in the Public Health Care Act of Turkmenistan, a new abortion law that effectively restricted access to abortion beyond five weeks, puts into risk many young girls who just hit puberty and have limited understanding of their menstruation cycle, not to mention understanding and preparedness for pregnancy.
Education on reproductive health and rights
When it comes to education on reproductive health and rights in Turkmenistan, alongside gender equality and life skills education is covered as part of the Basics of Life Skills mandatory subject for 7-10 grades in secondary schools. However, the education is abstinence-focused and does not cover contraception, sexuality education and gender-based violence. This means, the only feasible and realistic way to reach out to every adolescent in Turkmenistan and teach them about contraception and sexuality, lost its opportunity to be all-encompassing. In addition, the website of the Ministry of Education does not provide curriculum information and programs for schools, hence it is not clear what is in the government’s plan when it comes to sex education.
There are other projects that the government in Turkmenistan conducts in collaboration with UN organizations, such as three UNFPA-supported Peer Education Youth Centres, launched under the MoE and Youth Organisation in Ashgabat and Mary cities, that promote adolescent reproductive health and gender equality among others. The Y-PEER education and Yashlyk also deal with traditional sensitive issues, such as HIV/STIs, unwanted pregnancy, contraceptives, and gender-based violence. It is important to note that there are only a few Peer Education Youth centers and most are inaccessible to the majority and almost unknown to the public. The data on their activities are not shared to the public, making it difficult to assess the validity and its impact. But much like with the state subject Basics of Life Skills, UNFPA Turkmenistan tends to provide information in a similar fashion: mostly using the language of “reproductive health” and not “sexual education” in its content and materials.
This implies that the government of Turkmenistan with the support of UNFPA sees any sexual activity in the context of “reproduction” only, in the context of family and not outside of marriage, which is problematic, as the young population in Turkmenistan does not receive comprehensive sexuality education programs neither from the government nor from UNFPA and its affiliated centers for youth.
Photo: Y-PEER volunteers in Turkmenistan. Photo: UNFPA Turkmenistan